 Centre for Arthroscopy & Sports Orthopaedics
Centre for Arthroscopy & Sports Orthopaedics
Centre for Arthroscopy & Sports Orthopaedics
Centre for Arthroscopy & Sports Orthopaedics
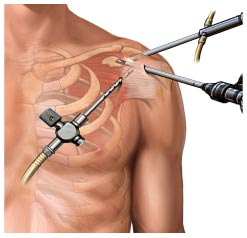
Arthroscopic (Key-hole) surgery is the technique of performing surgery though small (0.5-2cm) incisions rather than the larger incisions of conventional 'open' surgery. The operation uses telescope & camera to see inside the shoulder joint so that the surgeon can carry out the necessary procedure.
The advantages of arthroscopic surgery include less pain after the operation, smaller scars, lower risk of complications and a faster return to normal activities.
There are many conditions that may potentially require surgery. The doctor will explain your diagnosis, reasons for doing surgery as well as any alternatives. Whilst occasionally arthroscopy is used to help with the investigation of a shoulder condition, the diagnosis has usually been made by pre-operative examination and investigations.
The conditions commonly treated by shoulder arthroscopy include:Shoulder arthroscopy is almost always carried out under a general anaesthetic, meaning you will be asleep. The anaesthetic is sometimes supplemented with a nerve block (interscalene block) which involves an injection into the side of your neck which numbs the whole shoulder and most of your arm. This can be helpful for controlling pain after the operation.
Once under anaesthetic your shoulder will be re-examined. You will have two or three small incisions made (0.5 – 1cm long) at the back, side and front of the shoulder. Sometimes additional incisions need to be made. Your shoulder is then filled with fluid. An instrument known as an arthroscope (telescope) is passed into the shoulder. This is attached to the camera which allows your surgeon to look around your shoulder and using other specialised instruments to carry out your surgical procedure. The small incisions may/maynot usually require stitches and heal by 2 weeks. You will have a dressing applied and a Sling/Arm pouch as appropriate.
The majority of shoulder arthroscopy patients will go home 1-2 days after surgery. You will not be able to drive immediately after your surgery and will require someone at home to look after you at least for the first 48 hours.
You will be asked to follow-up regularly after your operation to assess your recovery.
Roughness of the under-surface of the Acromion (the bony tip of the shoulder) has caused rubbing and irritation to the soft tissues (bursa & tendon) which pass under this bone. This typically causes pain at the outer part of the shoulder and upper-arm, especially when lifting the arm above the shoulder height.
Treatment initially includes pain killers and physiotherapy, but occasionally these do not fully relieve the symptoms. This is when surgery is considered.
The subacromial decompression smoothens the bone allowing the soft tissues to move freely, relieving the pain.
The joint between the collar bone (clavicle) and the bony tip of the shoulder (acromion) is known as the acromio-clavicular joint (ACJ). This is a very common site for arthritis, where the protective cartilage wears away and allows the bones to rub against each other, causing pain. This pain is typically felt on the top of the shoulder and is worst reaching high above the head, or when crossing the arm across the chest.
Again, treatment initially includes pain killers and physiotherapy but when this does not fully relieve the symptoms surgery is considered.
The ACJ excision shaves away the end of the collar bone to allow more space between the collar bone and the shoulder tip. The space then fills in with scar tissue. This stops the bones rubbing, relieving the pain.
Frozen shoulder is a painful condition in which the flexible lining capsule of the shoulder joint thickens, becoming stiff and stuck to the other muscles and ligaments of the shoulder. It is not fully understood why this happens, but it can be associated with diabetes and injuries to the shoulder (including surgery).
Frozen shoulder usually settles of its own accord, but this can take upto two years. In the early stages, injecting the shoulder joint with local anaesthetic and steroid (cortisone) and physiotherapy are used to relieve the pain and improve the range of movement. In very severe cases, surgery is considered.
The surgery involves freeing up all the scarred, stuck portions of the capsule and manipulating the shoulder to ensure a full range of movement can be achieved. After the surgery, early mobilization of the shoulder is essential to maintain this movement.
Shoulder instability refers to the ball-and-socket joint not remaining securely in place. This can cause the shoulder to feel like it is coming out of joint either partially (subluxing) or fully (dislocating). This often happens after an injury.
In some cases, physiotherapy can train the muscles around the shoulder to balance the shoulder joint meaning it becomes more stable. However, when there is physical damage to the supporting structures in the shoulder (labrum, ligaments, capsule and bones) the shoulder is at high risk of remaining unstable. In these cases, surgery can be useful to repair those damaged structures. After surgery, it is important to protect the repair and as such you will be in an Arm pouch/sling for a few weeks.
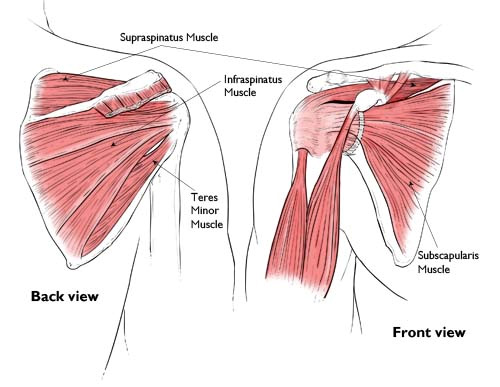
The rotator cuff is a group of four tendons that (with the associated muscles) form a deep layer of the shoulder. They help to lift the arm above the head and also to rotate the arm. The tendons run under the bony tip of the shoulder blade (acromion), where they are vulnerable to harm. This can either be damage in the form of gradual wear-and-tear, or injury from sudden trauma (or a combination of the two), both of which can cause a rotator cuff tear.
The symptoms of a torn rotator cuff include pain, typically down the side of the shoulder and arm. The pain is often worst at night and aggravated by lying on the affected side. The patient is also weaker in the affected shoulder, and often this means the arm cannot be lifted above the head.
The treatment for minor rotator cuff tears commences with painkillers and physiotherapy to keep the shoulder strong and supple. The strong outer layer of shoulder muscles can often be taught to compensate for the torn tendons, which brings symptoms under control.
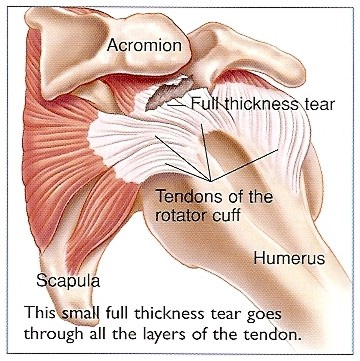
In case of > 50% partial or complete Rotator cuff tears, repairing the tendons is indicated through key-hole surgery. The aim of the surgery is to re-attach the torn tendon to the bone to allow the muscles to function properly once again. Small anchors with stitches attached are used to repair the torn rotator cuff tendon back to the bone.
After surgery, it is important to protect the repair and as such you may be in an Arm pouch/sling for few weeks depending on the extent of the tear.